Beyond the Battlefield: Towards a Better Assessment of the Human Cost of Armed Conflict
25 Sep 2017
By Erik Alda and Claire Mc Evoy for Small Arms Survey

This article was external pageoriginally published by the external pageSmall Arms Survey in September 2017.
Overview
Prevailing methods for measuring conflict deaths do not capture the total human cost of armed conflict.1 In the context of the UN’s 2030 Agenda for Sustainable Development, one global indicator will deal with conflict-related deaths. Various stakeholders have thus called for the monitoring of conflict deaths to become more holistic and go beyond battle deaths, specifically by covering indirect factors such as a lack of access to healthcare, food, and clean water. This Briefing Paper supports their call, arguing that the current understanding of—and measurement approaches to—conflict-related deaths should be broadened to include more comprehensive mortality figures from conflict zones, particularly among forcibly displaced populations. Its findings are designed to inform work towards meeting Target 1 of Sustainable Development Goal (SDG) 16, which commits all UN member states to significantly reducing ‘all forms of violence and related death rates everywhere’. Specifically, the paper is intended to help shape the development of SDG Indicator 16.1.2, which will guide the measurement of conflict-related deaths.
Key findings
- As part of the UN’s 2030 Agenda for Sustainable Development, the measuring of conflict deaths will initially focus on direct battlefield deaths, yet there is an opportunity to go beyond this to capture the full range of mortality from armed conflict—particularly among displaced populations.
- Various stakeholders, including international and non-governmental organizations in the health sector, have a key role to play in ensuring that the full range of conflict-related deaths is captured and understood.
- By capturing a broader scope of conflict-related deaths, stakeholders will be able to further the knowledge base around particular conflicts and better inform policies and programmes on conflict prevention, preparedness, and humanitarian response.
- In spite of significant barriers, recent efforts have secured some improvements in the techniques used to estimate indirect conflict deaths; additional progress could be made through the establishment of an international platform dedicated to furthering related methodologies and processes.
Introduction
Conflicts have become more lethal in the past decade (OECD, 2016, p. 35). Put differently, fatalities have risen sharply:
deaths caused by war-related injuries and attacks, such as those inflicted by a bullet, bomb, mine, machete, or assault, [increased] from an average of 55,000 in 2004–09, to 70,000 in 2007–12, and up to 90,000 in 2010–15 (Widmer and Pavesi, 2016, p. 4).2
The most lethal conflicts in 2015 were in Afghanistan, Iraq, and Syria, which have been the world’s deadliest war zones since 2012 (Widmer and Pavesi, 2016, p. 5).
While data on direct conflict deaths may be patchy, it is generally available. Sources include UN peacekeeping missions, international databases on conflicts, and casualty recorders.3 In contrast, an estimate of the number of deaths occurring indirectly in conflict settings—as a result of the effects of forced displacement, a breakdown of infrastructure, disease, and malnutrition—has remained elusive. These adverse conditions are typically compounded by the inability of government institutions and public health systems to overcome the multiple, negative, long-term effects of conflict. Meanwhile, methodological challenges limit our understanding of the root causes of indirect deaths and, by extension, how to prevent them.
Methods used to measure the broader scope of conflict-related deaths generally focus on excess mortality, or the difference between wartime crude mortality rates and the baseline or counterfactual mortality that would have occurred in the absence of conflict. Typically, retrospective mortality surveys, prospective surveillance through the health information system, and the analysis of multiple data sources are used to determine estimates. Although research has put forward various methodologies for measuring conflict-related deaths, ‘no validation mechanism has been developed to create consensus on which methods best capture the entire range of the phenomenon’ (Small Arms Survey, 2017, p. 1).
Limited efforts have been made to assess the ratio of direct conflict deaths to indirect conflict deaths (Geneva Declaration Secretariat, 2008, ch. 2; HSRP, 2011, ch. 5). In 2008, the Geneva Declaration Secretariat, hosted by the Small Arms Survey, estimated that since the early 1990s in conflicts where good data existed, ‘the burden of indirect deaths was between three and 15 times the number of direct deaths’ (Geneva Declaration Secretariat, 2008, p. 32). It proposed an average ratio of four indirect deaths for every direct death as a conservative global estimate (p. 42).
Attempts to assess the relationship between direct and indirect conflict deaths may soon be facilitated by the highly anticipated ‘data revolution’, a key aspiration of the 2030 Agenda (IEAG, 2014, pp. 4–10). As regards conflict settings, the official SDG monitoring process for Target 16.1— which focuses on reducing all forms of violence and related death rates—is advancing on ‘defining and identifying relevant conflict situations and conflict related deaths (direct and indirect)’ (IAEG, 2017a, p. 206). As described below, Indicator 16.1.2 under that target may initially be used to focus on measuring direct battle deaths. However, various stakeholders are calling for ways to consider a more comprehensive approach—one that would also capture indirect mortality in conflict settings.
Within the SDG framework, international organizations, civil society, and academics—including health sector professionals— have a key role to play in conflict zones, where state capacities to collect data are likely to be inadequate. With respect to assessing conflict-related mortality that includes indirect deaths, they can support and complement national data collection efforts by assisting in mapping exercises and analysis; they can also help to reconcile conflicting estimates and to overcome methodological challenges— such as those related to definitions, coverage, accuracy, reliability, and comparability (Small Arms Survey, 2017, p. 3). In this way, they can contribute to the knowledge base and enhance methodological techniques, for example by encouraging cross-checking among multiple sources. Such interaction is expected to inform resource allocation decisions, policy-making, and humanitarian preparedness and response programmes, while also bolstering accountability.
This Briefing Paper makes a case for stepping up efforts to measure and understand the entire range of conflict-related deaths, particularly among forcibly displaced populations. It explores the opportunities provided by the SDG framework, especially Target 16.1 and other health-related targets, and provides an overview of methods used to measure conflict-related deaths. Finally, it discusses the importance of developing more nuanced, context-specific methods for estimating the relationship between direct and indirect conflict deaths.
Conflict-related deaths in the SDG framework
The 2030 Agenda is the first universal framework to make an explicit connection between violence (and conflict) and development: ‘Sustainable development cannot be realized without peace and security; and peace and security will be at risk without sustainable development’ (UNGA, 2015, para. 35). Two SDGs are of particular relevance to the reduction of conflict-related violence:
- SDG 3 calls on states to ‘[e]nsure healthy lives and promote well-being for all at all ages’; and
- SDG 16 asks them to ‘[p]romote peaceful and inclusive societies for sustainable development, provide access to justice for all and build effective, accountable and inclusive institutions at all levels’.
Under SDG 16, Target 16.1 commits states to ‘[s]ignificantly reduce all forms of violence and related death rates everywhere’ and gives expression to the view that violence holds back development and human empowerment. As such, the target represents an opportunity to fill major data gaps and to make a difference in an area that was not recognized in the Millennium Development Goals (Alvazzi del Frate and De Martino, 2015, p. 4; Kleinfeld, 2017). Within this framework, states have committed to measuring progress using the following two indicators on violent deaths:
- Indicator 16.1.1: the ‘[n]umber of victims of intentional homicide per 100,000 population, by sex and age’; and
- Indicator 16.1.2: ‘[c]onflict-related deaths per 100,000 population, by sex, age and cause’ (IAEG, 2016, p. 34).
Indicator 16.1.2 has yet to be finalized. The Inter-agency and Expert Group on SDG Indicators, which is responsible for defining global indicators and the methodologies to measure them, has placed it in ‘Tier III’4, noting: ‘There is no established methodology for the indicator’ (IAEG, 2017b, p. 26). The possible custodian agency for the indicator, the Office of the United Nations High Commissioner for Human Rights (OHCHR), is likely to take a phased approach to measurement, focusing initially on violent deaths in conflict settings. The question of non-violent conflict-related mortality will be addressed only in a second step.5 This approach reflects the fact that, despite a host of challenges, direct conflict deaths are more measurable than indirect conflict deaths.
Figure 1 Selected causal chains from armed conflict to indirect conflict deaths
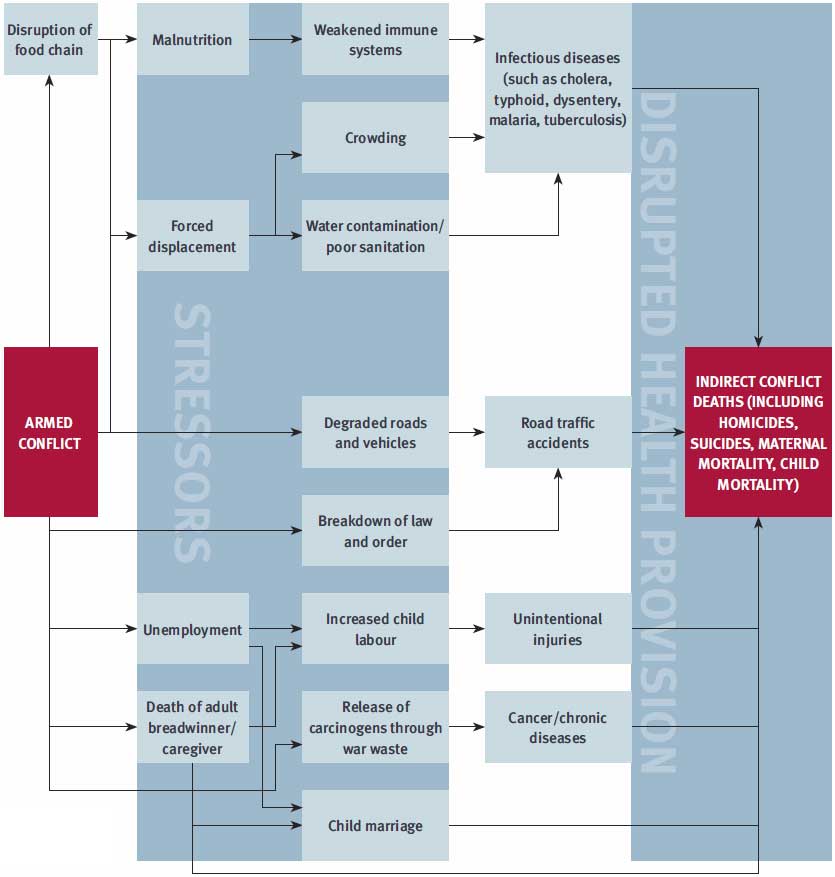
Understood as non-violent mortality that exceeds levels that could have been expected in the absence of war, indirect conflict deaths result from a variety of specific causes linked to the worsening of social, economic, and health conditions in conflict-affected areas (Geneva Declaration Secretariat, 2008, p. 33).6 In contrast to direct conflict deaths—with a few exceptions, such as lives lost due to land mines or unexploded ordnance— indirect deaths can occur both during and well after the end of hostilities.
By calling for data that is disaggregated by sex, age, and cause, Indicator 16.1.2 is expected to help fill persistent knowledge gaps. Data collected under this indicator will inform policy-makers on how, when, and where conflict-affected people—both male and female—are dying.7 Similarly, the collection of qualitative data on causes of death will serve to provide a fuller picture of the causal chains that lead to indirect conflict deaths—a first step in trying to prevent them (see Figure 1).
Recent research demonstrates that ‘our ability to prevent or mitigate the indirect human toll of war has made unprecedented progress’ (Wise, 2017, p. 139). Indeed, suitably targeted remedial actions—such as vaccination campaigns, food distributions, and improvement of water and sanitation services—regularly prevent people in conflict-affected regions from dying. Nevertheless, lives continue to be lost wherever such interventions are inadequate, arrive too late, or fail to materialize.
Box 1 SDG 3 and conflictrelated deaths
SDG 3 indicators call for a wealth of mortality data that can help to assess the impact of conflict on societies:
- Indicator 3.1.1: maternal mortality ratios;
- Indicator 3.2.1: under-five mortality rates;
- Indicator 3.2.2: neonatal mortality rates; and
- Indicator 3.9.2: mortality rates attributed to unsafe water, unsafe sanitation, and a lack of hygiene (IAEG, 2016, pp. 17–19).
In this context, causal chains can serve as a useful tool, as they can reveal what types of interventions may be required to save lives (Widmer, 2017b, p. 11). A more systematic examination of these chains could help in the identification of less intuitive links. A spike in accidental deaths in the workplace, for example, may be linked to an increase in child labour, which may be due to the absence of adult breadwinners, if parents have died in battle or in other conflict-related ways. Similarly, child marriages due to absent adult breadwinners may lead to an increase in maternal mortality.
SDG 3 is particularly relevant to this discussion as it endeavours to ‘[e]nsure healthy lives and promote well-being for all at all ages’. It mandates the monitoring of deaths from a number of communicable and non-communicable conditions that are highly relevant in conflict and post-conflict situations. Four SDG 3 indicators are particularly pertinent to the measurement of conflict-related deaths (see Box 1). Other measurements of health-related quality of life in conflict situations are also relevant, specifically under:
- SDG 2: ‘End hunger, achieve food security and improved nutrition and promote sustainable agriculture’; and
- SDG 6: ‘Ensure availability and sustainable management of water and sanitation for all’ (IAEG, 2016, pp. 16–19, 22–23).
Government-led national statistical offices will be central to SDG-related data collection efforts and reporting. States that are experiencing armed conflict may be constrained in their capacity or willingness to collect data; if governments are parties to conflict, reporting bias may be an issue.8 Other actors—such as international organizations, academic institutions, and civil society—thus need to support or complement national efforts to measure the broader impact of armed conflict. If these different actors—be they from the humanitarian, development, political, or health sector—undertake actions in consultation and coordination with each other, they will be in a better position to meet the needs of conflict-affected populations, including displaced people (see Box 2). In view of the major impact conflict has on public health, researchers face the daunting challenge of identifying data collection methodologies that can be applied in conflict situations.
Box 2 Conflict-related deaths among displaced populations
The past two decades have seen an explosion in the number of forcibly displaced people around the globe: from 37.3 million in 1996 to 65.6 million by the end of 2016 (UNHCR, 2016, p. 6; 2017, p. 2). During 2016 alone, 10.3 million people were newly displaced by conflict or persecution (UNHCR, 2017, p. 2).9 The vast majority of internally displaced persons (IDPs, 99 per cent) and refugees (89 per cent) live in developing countries, where health infrastructure may be wanting or unavailable (World Bank, 2017, p. 18).
In the absence of humanitarian assistance, forcibly displaced populations can be at particular risk of dying from causes indirectly related to conflicts. Excess mortality rates are especially high among IDPs in conflict areas (Heudtlass, Speybroeck, and Guha-Sapir, 2016, p. 1).10
The institutional, economic, and social breakdown resulting from conflicts often affects men, women, and children differently. While men are more likely to die during conflict, women and children account for the majority of refugees and forcibly displaced people (Strachan and Haider, 2015, p. 11). Research also shows that deteriorating conditions due to conflict negatively affect reproductive health and maternal mortality, leading to higher death rates among women and children (Chi et al., 2015).
The consequences of displacement include unemployment, exposure to communicable diseases—most commonly cholera, typhoid, hepatitis, and dysentery—a lack of access to public health and educational systems, neonatal and pregnancy-related complications, and food insecurity. These specific vulnerabilities may or may not be shared by host populations.
Unless the monitoring of conflict-related deaths covers IDPs and refugees, fatalities among forcibly displaced populations may not be recorded as indirect conflict deaths. In the absence of data on these deaths, policies, programming, and funding for conflict prevention, peacebuilding, and humanitarian aid for conflict-affected populations will be based on incomplete and possibly misleading information.
Measuring indirect conflict deaths
One of the best-known methods for determining conflict-related deaths is through the measurement of excess mortality. It is calculated using a crude mortality rate (CMR),11 which is only useful when it can be juxtaposed with a baseline CMR.12 The difference between the ‘crisis CMR’ and the ‘baseline CMR’ provides the excess mortality for a given crisis.13 It can be broken down into two types of conflictrelated deaths—direct and indirect— according to whether the cause of death was violence. Thus, indirect conflict deaths can be calculated by subtracting direct conflict deaths and baseline mortality from the CMR.
Conflict death monitoring in conflict zones rarely yields data on indirect conflict deaths, however. Of the organizations that publicly track fatalities in Syria, for example, the Syrian Center for Policy Research is the only one that distinguishes between violent and indirect deaths (SCPR, 2016, p. 45).14 If data does not indicate the cause of death, it cannot be used to estimate conflict-related excess mortality.
Furthermore, the accuracy of excess mortality estimates depends on the availability and reliability of the baseline mortality data. In many conflict zones the establishment of a baseline is rendered difficult, if not impossible, by the absence of reliable pre-conflict data. Baseline estimates tend to be contested; depending on the chosen methodology, researchers may reach different results. Determining an average ratio to describe the relationship between violent and non-violent conflict deaths is thus particularly challenging, as discussed in the next section.
Developing a ratio of direct to indirect conflict deaths
Ratios of violent to indirect conflict-related deaths can prove useful for estimating the scale of conflict-related humanitarian crises. To arrive at suitably refined ratios for specific populations that are experiencing armed conflict or transitioning to peace, researchers should develop estimation techniques that take into account a host of local factors. In this process, it is critical to consider what can break the causal chains that lead to indirect deaths, such as the availability of humanitarian interventions aimed at providing medicine, food, and shelter, or an operational local health system (HSRP, 2011, p. 105). Other factors that should be taken into account include the intensity and length of a conflict; the sex and age of the victims; and seasonal or climatic trends. By reflecting changes on the ground, the resulting ratios would dramatically improve stakeholders’ understanding of the links between direct and indirect deaths, and thus their ability to save lives, both during a conflict and once hostilities have died down.
It is difficult to determine a reliable ratio, however, if both baseline and conflict-related death tolls remain elusive. The Darfur conflict in western Sudan provides an example of the challenges of measuring conflict-related deaths—direct and indirect—and of the debates within the international community about the reliability of various results (see Box 3). There has been similar disagreement in relation to estimates for other conflicts, such as in the Democratic Republic of the Congo, Iraq, and Syria (Science, 2010; Spagat and van Weezel, 2017; Taylor, 2016).
Further methodological considerations
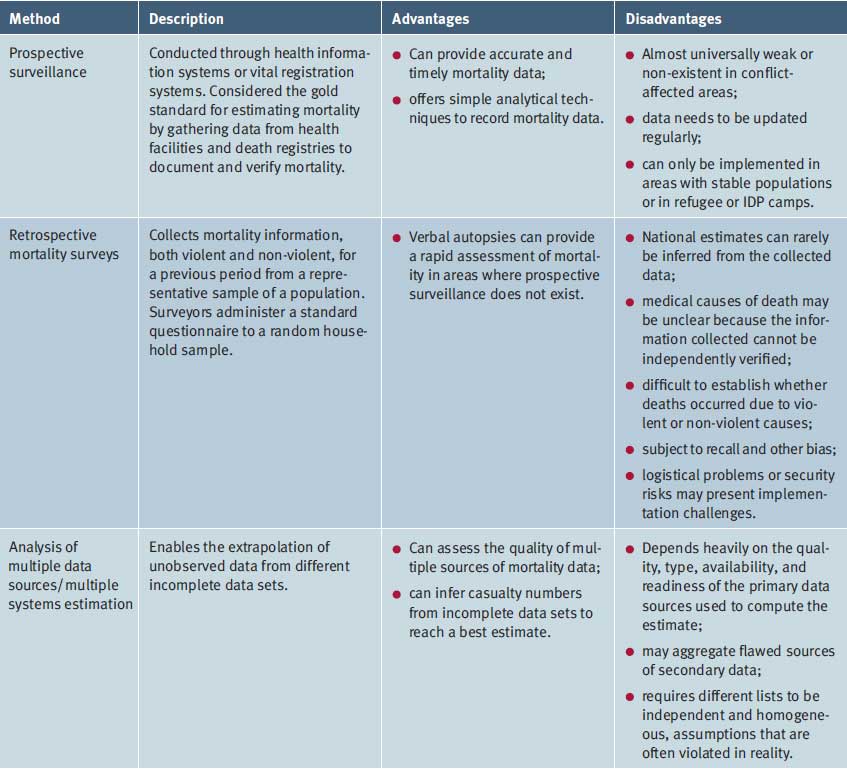
Varying methodologies and statistical techniques are used for data collection and analysis of conflict-related deaths. This section discusses three different methodological approaches: prospective surveillance, retrospective mortality surveys, and analysis of multiple data sources; Table 1 presents a summary of their advantages and disadvantages. While each method has inherent strengths, researchers should assess the local context and employ single or combined methodologies that are best suited to a particular environment.15
Prospective surveillance
The prospective surveillance of mortality through a health information system or vital registration system is the gold standard for estimating mortality. By collecting data from health facilities and death registries to document and verify mortality, these systems can provide accurate and timely data. Ad hoc surveillance within humanitarian operations and in areas hosting IDPs may also provide assistance, although their figures are prone to under-reporting due to the absence of accurate demographic information (Heudtlass, Speybroeck, and Guha-Sapir, 2016, p. 6).
Box 3 Estimating ratios in practice: the case of Darfur16
A wide range of research illustrates the methodological challenges involved in measuring conflict-related deaths by cause, estimating total numbers of conflict-related deaths, and calculating proportions of direct conflict deaths to indirect deaths (Geneva Declaration Secretariat, 2008, ch. 2; Levy and Sidel, 2016). The absence of a baseline against which to compare can represent a major obstacle.
The Darfur conflict17 has been studied extensively to provide estimates of its human cost. Most initial estimates of the death toll from the Darfur conflict were based on two early data sources: (1) a World Health Organization (WHO) mortality survey of internally displaced populations primarily in West and North Darfur; and (2) interviews with Darfuri refugees in Chad, conducted for the most part by independent experts recruited by the Coalition for International Justice (CIJ).
The WHO survey was conducted in August 2004 in IDP camps in North and West Darfur, plus one additional camp in South Darfur, with a recall period of two months (WHO, 2004, p. 4). The survey found that approximately 14 per cent of reported mortality was due to violence, although this result has to be interpreted cautiously as respondents also stated that household members were ‘absent’ or had ‘disappeared’—and this data was not included in the 14 per cent. Moreover, the survey did not posit a baseline mortality rate and hence not all of the non-violent deaths—the remaining 86 per cent—can be presumed to be conflict-related (WHO, 2004).
In July and August 2004, the CIJ conducted 1,136 qualitative interviews with Darfuri refugees in eastern Chad (USDOS, 2004). The following year, the CIJ combined the results of those interviews with the WHO findings to extrapolate a figure of almost 400,000 conflict-related deaths for the whole of Darfur, including among refugee populations in Chad. The researchers estimated that one-third were direct conflict deaths, which translated into two indirect deaths for every violent death (CIJ, 2005). The interviews were not designed as a mortality survey, however; nor did they adopt a robust sampling methodology, raising questions about the validity of the ratio (USGAO, 2006, p. 58). In January 2005, an independent researcher undertook a separate review of all available data sets. The analysis inferred a total of some 300,000 excess deaths between February 2003 and December 2004, of which just over half were reportedly direct—violent—conflict deaths, thus yielding a ratio of 1:1 (Coebergh, 2005).
In another study conducted in 2005, researchers at the Centre for Research on the Epidemiology of Disasters (CRED) combined data from 24 small-scale surveys carried out between April 2004 and January 2005 in Darfur and eastern Chad (Guha-Sapir and Degomme, 2005, p. 14). Based on this data set, they extrapolated that the excess deaths due to the conflict between September 2003 and January 2005 numbered 118,000, of which 35,000 were reportedly violent. These findings translate into 2.4 indirect conflict deaths for every violent death. The authors note that non-violent mortality was particularly high between June and August 2004, corresponding to the ‘hunger season’ in Darfur (p. 8).
In 2006 yet another study combined the data sets generated in 2004 by WHO and the CIJ, as well as a Medecins Sans Frontieres survey (Depoortere et al., 2004); the result was a new set of estimates of monthly mortality in Greater Darfur (Hagan and Palloni, 2006). The authors traced the evolution of crude mortality rates between September 2003—after eight months of conflict—and July 2005—after 30 months of conflict. According to their estimates, direct (violent) deaths exceeded indirect ones during the entire period, although they were nearly equal by mid-2005. The authors note, however, that crude mortality rates from violence may have been overestimated and that deaths from indirect causes may have been underestimated. Furthermore, they did not deduct any hypothetical baseline mortality from the rates of direct and indirect mortality; their estimate was therefore not limited to excess mortality from conflict.
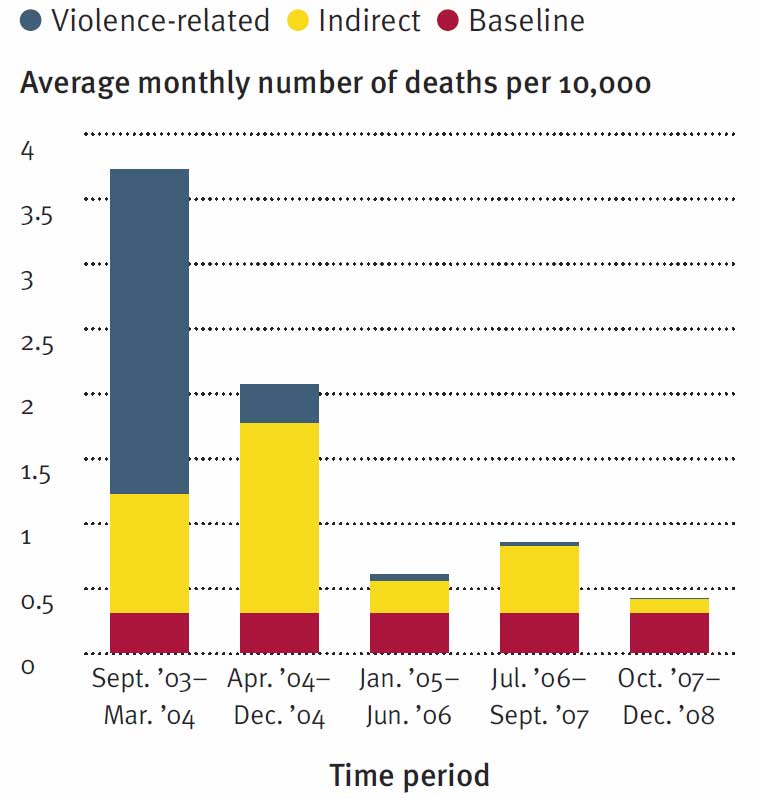
In 2010, Degomme and Guha-Sapir incorporated an even larger number of surveys into a study, combining data from 107 local and national retrospective mortality surveys to analyse trends in violence- and diarrhoea-related mortality from September 2003 to December 2008 (Degomme and Guha-Sapir, 2010, p. 295). Their findings show that, depending on the chosen baseline value, 70–80 per cent of excess deaths over the entire period did not result from violence. This conclusion suggests a ratio of 2.4 to 3.8 indirect conflict deaths for every violent death. Significantly, the ratio varied widely during different phases of the conflict (p. 298). Figure 2 presents average mortality rates throughout the war, assuming a constant baseline mortality of 0.3 deaths per 10,000 per day and treating all violent deaths as excess mortality.
If these assumptions are correct, the initial, acute phase of the war witnessed almost three times more violent deaths than indirect conflict deaths. Direct conflict deaths decreased sharply in April 2004, while indirect mortality was still on the rise: between April and December 2004, Darfur registered four to five non-violent excess deaths for every violent death. These findings depart from an earlier extrapolation by Hagan and Palloni (2006), which had found that direct mortality still exceeded indirect deaths during this period. Degomme and Guha-Sapir’s calculations indicate that from mid-2006, indirect conflict deaths exceeded direct conflict deaths by a factor of ten or more.18
The research conducted by Degomme and Guha-Sapir suggests that indirect conflict deaths do not directly correlate with direct (violent) deaths. Rather, they seem to be dependent on the scale of recent displacement and the availability of humanitarian aid.
Retrospective mortality surveys
When the direct collection of mortality data is not possible, household surveys known as retrospective mortality surveys (RMSs) can be used to ask respondents about information on past violent and non-violent deaths.
The advantage of an RMS is the rapid assessment of mortality in areas where prospective surveillance does not exist. RMSs provide better estimates than multiple systems estimation (see below) for indirect conflict deaths from famine or illness (Klingner and Silva, 2013, p. 159). An example of the practical application of this method is a study by Silva and Ball (2008), which estimates an excess number of deaths of approximately 84,000 during the Indonesian occupation in Timor-Leste due to famine and illness, compared to the number of deaths expected during peaceful times.
While survey methodologies and statistical techniques have improved significantly in recent years in terms of collecting and analysing data in difficult contexts, they still suffer from limitations. Reflecting particularly difficult conditions for data collection, these limitations include poor-quality data and small samples that cannot be extrapolated to the whole population. Other shortcomings that can affect overall data quality include insufficient training of interviewers, inadequate supervision, and substandard quality control.19
Furthermore, RMSs are sometimes undertaken on a localized basis and national estimates can rarely be inferred from the data collected in, for example, refugee and IDP camps (HSRP, 2011, p. 108). Researchers can partially correct this weakness by aggregating several small-scale surveys and by controlling for well-known survey bias. Logistical problems or security risks may make RMSs challenging to implement, especially since the data generated may be politically sensitive. The information on deaths may also be impossible to verify independently.
Nevertheless, RMSs remain a useful tool in conflict situations with little or no previous mortality information and are appropriate for estimating indirect conflict deaths. RMS methods have been standardized through an inter-agency humanitarian initiative (WGMEE, 2007).
Figure 2 Average crude mortality rates and excess mortality in Darfur, September 2003–December 2008 (cumulative)
Analysis of multiple data sources
Due to the abovementioned challenges, most data sets on mortality from conflict situations are incomplete and may be biased to various degrees. They can, however, be usefully combined to derive more accurate estimates of wartime mortality, wartime excess mortality, and the proportion of direct and indirect (that is, violent and non-violent) mortality (Widmer, 2017b, p. 9).
The analysis of multiple data sources permits the reconstruction of mortality profiles using data collected before, during, and after a conflict. Multiple systems estimation (MSE) techniques are complex statistical methods that enable, in principle, the extrapolation of unobserved data from different sets of data (Widmer, 2017b, p. 9). The clear advantage of MSE is the ability to derive a best estimate from multiple sources, for example based on two or more incomplete casualty lists (Seybolt, Aronson, and Fischhoff, 2013, p. xvi). Data sources can include incomplete prospective surveillance data and ad hoc surveillance data, including from humanitarian operations, eyewitness and media reports, administrative records, and lists of missing persons (Obermeyer, Murray, and Gakidou, 2008).
MSE is most useful if survey instruments are used in addition to casualty lists, as this approach can help to link cases, as well as to answer in-depth research questions, including estimations of direct and indirect mortality deaths (Klingner and Silva, 2013, p. 159). MSE encompasses models that can lead to very different estimates of total casualty numbers from the same set of lists, however. The approach can also aggregate potentially flawed sources of secondary data, which may lead to inaccurate results. Furthermore, the technique requires different lists to be independent and homogeneous, assumptions that are often violated in reality.20 During the tenure of the Truth and Reconciliation Commission in Peru, for instance, analysts expected the homogeneity assumption to be violated. Researchers had to adjust the sample to conduct the analyses (Manrique-Vallier, Price, and Gohdes, 2012, p. 177).21
Table 1 Review of methods to quantify indirect conflict deaths
Nevertheless, the use of MSE techniques to estimate conflict-related mortality is on the rise. In Casanare, Colombia, a research team employed the MSE approach—using 15 sources of data—together with a Bayesian framework22 to estimate the number of killings and disappearances that took place during the conflict from 2000 to 2007; they estimated that about 4,000 to 10,000 killings had occurred (Guberek et al., 2010, p. 3). A recent study on MSE methods concluded that these had evolved significantly in recent years to address ‘real-life’ problems and that MSE methods were ‘a versatile tool that enables the principled use of data frequently found in practice, and as such should be considered part of a standard “casualty-estimation toolbox”’ (Manrique-Vallier, Price, and Gohdes, 2012, p. 179).23
As MSE gains acceptance, particularly for exploring under-reported events in the human rights field, organizations such as the Human Rights Data Analysis Group are using the techniques to estimate detention in Syria and civilian casualties of war—both documented and undocumented—in Colombia, Guatemala, Kosovo, Peru, and Timor-Leste (Price, Gohdes, and Ball, 2016). The challenge is to continue to develop these methods to enhance their ability to capture indirect conflict deaths.
Opportunities ahead
In spite of significant barriers, recent efforts have secured some improvements in the techniques used to estimate indirect conflict deaths and a growing number of voices are calling for methodological advances to measure them more accurately.24 As discussed below, the SDG framework presents opportunities for overcoming methodological and data collection limitations (see Box 4).
Box 4 A plan of action for capturing conflict-related deaths
In January 2017 the Small Arms Survey convened an expert meeting to identify options for better capturing the burden of conflict-related deaths.25 Participants explored how the data collection framework of the 2030 Agenda could help the process and developed a plan of action to contribute to the advancement of relevant knowledge (Small Arms Survey, 2017). This step was taken in response to calls from a wide range of stakeholders involved in crisis mitigation and prevention who had made the case for capturing the comprehensive burden of conflict-related deaths. The meeting participants agreed that progress in this regard was necessary in order to realize goals in the context of the 2030 Agenda, the Agenda for Humanity,26 and the vision of sustained conflict prevention promoted by the UN Secretary-General and the UN Security Council.27
Participants recognized that the quantity and quality of data available on conflict-related deaths had improved noticeably over time but that several limitations persisted. These included the absence of a consensual definition of ‘armed conflict’, some state actors’ rejection of the term, and others’ attempts to influence reporting to strengthen a particular political narrative or influence policy-making.
The experts noted that future estimates should systematically disaggregate conflict mortality by cause, time, and affected demographic group in order to help provide an understanding of trends and risks. They also concurred that causal chains leading to violent and non-violent deaths would need to be investigated further in order to identify factors that should be considered in the design of policy responses.
They proposed the creation of a platform or ‘go-to place’—an interface with the official SDG measurement process that would allow all interested parties to discuss relevant information. Looking forward, participants agreed on the need to:
- Clarify the scope of conflict-related deaths. In recognition of the fact that definitions of armed conflict and its impacts are a prerequisite for identifying units of analysis and ensuring uniform accounts of conflict-related mortality, the group suggested developing a broad definition of ‘armed conflict’ with clear inclusion and exclusion criteria— including to help differentiate between conflict-related deaths counted under SDG Indicator 16.1.2 and non-conflict deaths counted under Indicator 16.1.1.
- Develop estimates of conflict-related mortality. The main tasks ahead will be to map, analyse, and reconcile different estimates of conflict-related mortality, both violent and non-violent, so that policy-makers may be provided with clearer estimates. Data sources may include casualty-recording databases, epidemiological or demographic studies of mortality, and indirect data sources, such as displacement figures or statistics from aid agencies. Interested participants are encouraged to undertake case studies. The role of the platform would be to ‘provide a scientific basis for the reconciliation and validation of particular estimates’, which would support methodological advancement.
Source: Small Arms Survey (2017, pp. 1–3)
Improving data and methodology
The accuracy of the estimates used to measure progress against any indicator depends entirely on the quality of the data collected. If data is deficient, estimates based on it are also likely to be deficient, regardless of the sophistication of the methodologies used. Moving forward, the international community’s efforts to improve and standardize survey quality may contribute to overcoming some of the limitations inherent in gathering and analysing data on indirect conflict deaths. Efforts to improve standards for sampling and survey methods will also be driven by the emphasis placed on survey-related indicators for measuring the SDGs.28
Beyond the most popular methodologies, it is important to take into account advances in Bayesian methods, which can yield credible and robust estimates in data-poor environments (Alkema and New, 2014, p. 21). In addition, statistical techniques such as structural equation models (SEMs)29 and causal mediation analysis30 can also yield useful estimates on the direct and indirect causes of deaths. For example, a 2012 study using a SEM model focused on the indirect effects of war, hunger, and disease on the reduction of life expectancy in a sample of countries in sub-Saharan Africa (Austin and McKinney, 2012, p. 421).
Developing more nuanced ratios
Current estimates based on one single ratio may defeat the purpose of disaggregating data by age, cause, sex, and specific contextual factors. While a harmonized range of ratios that captures the various factors that lead to indirect conflict deaths may not solve this problem entirely, it could offer a more comprehensive assessment of the burden of conflict-related deaths, especially in data-poor contexts.
More accurate ratios—ones that consider the leading causes of non-violent mortality in conflict situations and recognize the particularities of different contexts and the shifting phases of conflict—are needed in order to better understand how to prevent indirect conflict-related deaths. They will also help to prevent potential issues related to ‘isomorphic mimicry’—such as policymakers arriving at decisions based on generally accepted views, rather than on data or evidence (Pritchett and de Weijer, 2010). Fragile and conflict-affected countries may adopt policies and programmes to maintain legitimacy with ‘sovereigns’ such as international organizations and donors, for example, without having the institutional capacity to implement these policies or programmes.31
Moving the agenda forward
Expanding the definition of conflict-related deaths will require agreement on how best to utilize the set of SDG indicators that can capture these deaths, as well as on how to track these fatalities in conflict zones. This work will necessitate consensus-building among all relevant actors and the mobilization of support for a possible phased approach to Indicator 16.1.2.
Improving data collection and analysis will require the use of new and old methodologies to collect and analyse data. This means designing new and improved, previously vetted survey instruments to collect data. Data warehouses may provide a platform upon which to build. One such initiative is the discontinued Conflict Emergency Database, which contains data from 3,432 surveys conducted by humanitarian organizations in more than 50 countries and territories since 2003 (CRED, n.d.).
Conclusion
Any assessment of how well the international community has performed in terms of satisfying SDG Target 16.1 needs to be empirically demonstrable, within and beyond the official monitoring framework. A failure to consider the full scope of conflict-related deaths may hide the real consequences of the complex emergencies unfolding across the globe today.
Moving forward, obtaining more comprehensive data on conflict-related deaths will require investment in data collection systems that focus not only on government-generated data, but also on improving survey systems, building on and amending relevant data sets, and generating new analytical methodologies that can capture the relationship between direct and indirect conflict deaths.
Multiple actors have a strong role to play in defining and expanding the scope of conflict-related deaths. The very same actors can assist national governments and their statistical offices in building their capacity to collect data, track progress against targets, and empirically validate the data. They can also assist governments wherever the capacities of national statistical offices are limited, as is often the case in conflict situations. Achieving this objective will require key international actors to talk to each other and to agree upon a set of steps that will lead to progress in this regard.
To date, efforts to measure conflict-related deaths have been scattered and driven by institutional and individual interests rather than a common interest. A dedicated research platform with a clear mandate could serve as an opportunity to develop this approach; to develop more nuanced ratios on the basis of case studies; to advance and develop related methodologies; to triangulate and validate different methods; and to unpack causal chains that lead to conflict deaths. Such a work plan would require the participation of core members and sufficient resources to facilitate the complex task of collecting and analysing mortality data in conflict environments. It would complement and take advantage of the official SDG data collection process and ultimately lead to more informed decision-and policy-making.
List of abbreviations
CIJ
Coalition for International Justice
CMR
Crude mortality rate
CRED
Centre for Research on the Epidemiology
of Disasters
IDP
Internally displaced person
MSE
Multiple systems estimation
OHCHR
Office of the United Nations High Commissioner
for Human Rights
RMS
Retrospective mortality survey
SDG
Sustainable Development Goal
SEM
Structural equation models
WHO
World Health Organization
Notes
1 Complicating matters, there is no international, consensual definition of ‘armed conflict’.
2 Data from Uppsala University shows that since 2015—following a peak in 2014—the rate of direct conflict deaths has been declining. Nevertheless, 2016 was ‘the fifth worst year seen over the entire post-Cold War period’ (Uppsala University, 2017).
3 See Pavesi (2017) for a review of monitoring systems that track conflict-related deaths.
4 A ‘Tier III’ categorization means that no internationally established methodology or standards are available yet for the indicator, but that these are being (or will be) developed.
5 In preparation for an expert meeting to be held in Geneva in September 2017, OHCHR noted the possibility that work would focus on measuring direct conflict deaths before expanding to include indirect conflict deaths (Small Arms Survey telephone conversation with an OHCHR official, 23 June 2017).
6 It should be noted that conflict is also associated with increased rates of homicide, suicide, and unintentional but fatal injuries, which blurs the distinction between violent and non-violent deaths. See Ghobarah, Huth, and Russett (2003, pp. 198–99).
7 Disaggregation by time period is not specified in SDG Indicator 16.1.2 but is arguably implicit.
8 A government that is engaged in conflict may under-report deaths in an area it administers or exaggerate fatalities in areas held by opponents, for example.
9 The UN Refugee Agency reports that the ‘number of new displacements was equivalent to 20 people being forced to flee their homes every minute of 2016’ (UNHCR, 2017, p. 2).
10 A recent study points to a need for further research ‘to clarify whether low estimates of excess mortality in refugees are the result of successful humanitarian interventions or due to the limitations of our methods and data’ (Heudtlass, Speybroeck, and Guha-Sapir, 2016, p. 1).
11 The CMR is the ‘number of deaths in a given period divided by the population exposed to risk of death in that period’ (OECD, n.d.).
12 Baseline mortality is a hypothetical mortality rate that can be extrapolated from a number of data sources, including: pre-war mortality data from health information or vital registration systems; total death estimates from databases of agencies such as the UN Population Division; data from a neighbouring country that has similar characteristics but is at peace; a regional average mortality rate; survey data exploring a pre-war period; and subnational wartime mortality data from a region that is not exposed to armed conflict (Widmer, 2017b, p. 8).
13 A humanitarian emergency is defined as any situation in which the CMR is double the baseline rate (Sphere Project, 2011, p. 310).
14 The distinction between indirect and direct conflict deaths is not made in data collected by the Syrian Network for Human Rights, the Syrian Observatory for Human Rights, or the UN special envoy for Syria.
15 See LSHTM (n.d.) for an overview of relevant epidemiological tools than can be used among conflict-affected populations.
16 This case study draws on Widmer (2017a). The provided ratios are extrapolations based on the cited research.
17 In contrast to attacks on villages in Darfur, which have a long history, large-scale violence broke out in early 2003, when rebel groups led assaults on the Khartoum government, which in turn armed local Arab and tribal militias to attack civilians. By January 2009, 2.7 million of Darfur’s population of 6 million had been internally displaced; the large scale and protracted nature of the displacement meant that many camps had effectively become urban settlements (IDMC, 2010, pp. 6, 11).
18 It should be noted that the baseline was based on an assumption. The authors also indicate that the proportion of violent deaths was lower in samples with many displaced individuals. In comparison to fatalities among non-displaced individuals, fewer displaced persons per capita died from attacks, but more died from communicable diseases (Degomme and Guha–Sapir, 2010, p. 298). As the surveys undertaken in IDP settings were over-represented in their sample, the authors tried to correct this bias in their analysis by weighting the results accordingly.
19 See LSHTM (n.d.) and UNDESA (2011) for a review of challenges.
20 ‘Independence’ means that a death captured by one list is not more or less likely to be captured by another list. This assumption would be violated if, for example, different casualty recording systems exchanged information on the cases they captured, or if some deaths were more likely to be recorded by non-governmental or governmental sources. ‘Homogeneity’ means every individual death is equally likely to be captured by a list. This assumption would be violated if, for example, deaths occurring in urban areas were more likely to be picked up than those occurring in rural areas. The other two assumptions underpinning MSE are a closed system, meaning different lists capture deaths from the same population—so if only one of the two lists includes crossborder refugees, this assumption is violated—and perfect matching, meaning that every single death can be identified precisely to determine which lists captured it and, hence, to what extent the lists overlap.
21 The sample was stratified to highlight or capture a particular subgroup by geographic location.
22 Bayesian methods are probability-based models that provide researchers with tools to update their estimates based on new data (Glickman and Van Dyk, 2007).
23 See also Kruger and Lum (2015), who applied MSE to estimate lethal violence in Kosovo for the period March–June 1999.
24 See Levy and Sidel (2017, p. 216), calling for a ‘an independent, nonpartisan mechanism, established and maintained by a United Nations agency or a multilateral organization, to investigate, document, and report on the health consequences of armed conflict’. This mechanism needs to include ‘the development, evaluation, and improvement of methodologies to document these consequences’.
25 Participants included representatives from American University, CRED, the Graduate Institute for International and Development Studies, the International Committee of the Red Cross, OHCHR, the Peace Research Institute Oslo, REACH/IMPACT, and the Small Arms Survey (Small Arms Survey, 2017).
26 A core responsibility identified in the Agenda for Humanity is to prevent and end conflict (WHS, 2016, p. 3).
27 See UNSG (2017) and UNSC (2017).
28 Several global indicators for monitoring progress in the context of the 2030 Agenda are survey-based. For example, data for Indicator 16.1.3—which covers the proportion of a population ‘subjected to physical, psychological or sexual violence in the previous 12 months’—will be collected through sample surveys of the adult population (IAEG, 2017c).
29 SEM models allow researchers to estimate the direct effects of conflict (battle deaths) as well as the indirect ones (deaths that result from the conflict-related breakdown of social and institutional structures).
30 Causal mediation analysis is similar to SEM but allows researchers to explore causal pathways and go beyond the estimation of a simple causal effect.
31 The adoption of ‘aid orthodoxy’ in South Sudan led to a massive aid effort to try to build the country and its institutions using best practices from other contexts. These efforts, while well intended, did not consider the fact that Sudan’s fragile institutional capacity precluded undertaking reforms (Larson, Ajak, and Pritchett, 2013).
References
Alkema, Leontine and Jin Rou New. 2014. ‘Global Estimation of Child Mortality Using a Bayesian B-Spline Bias-Reduction Model.’ Annals of Applied Statistics, Vol. 8, No. 4, pp. 2122–49 (subscription).
Alvazzi del Frate, Anna and Luigi De Martino. 2015. Every Body Counts: Measuring Violent Deaths. Research Note No. 49. Geneva: Small Arms Survey. March.
Austin, Kelly and Laura McKinney. 2012. ‘Disease, War, Hunger, and Deprivation: A Cross-National Investigation of the Determinants of Life Expectancy in Less-Developed and Sub-Saharan African Nations.’ Sociological Perspectives, Vol. 55, No. 3, pp. 421–47.
Chi, Primus Che, et al. 2015. ‘Perceptions of the Effects of Armed Conflict on Maternal and Reproductive Health Services and Outcomes in Burundi and Northern Uganda: A Qualitative Study.’ BMC International Health and Human Rights, Vol. 15, No. 7.
CIJ (Coalition for International Justice). 2005. ‘New Analysis Claims Darfur Deaths Near 400,000.’ Press release. 21 April. Washington, DC: CIJ.
Coebergh, Jan. 2005. ‘Sudan: Genocide Has Killed More than the Tsunami.’ Parliamentary Brief, Vol. 9, No. 7. London. February, pp. 5–6.
CRED (Centre for Research on the Epidemiology of Disasters). n.d. CE-DAT: Complex Emergency Database.
Degomme, Olivier and Debarati Guha-Sapir. 2010. ‘Patterns of Mortality Rates in Darfur Conflict.’ Lancet, Vol. 375, No. 9711, pp. 294–300.
Depoortere, Evelyn, et al. 2004. ‘Violence and Mortality in West Darfur, Sudan (2003–04): Epidemiological Evidence from Four Surveys.’ Lancet, Vol. 364, No. 9442, pp. 1315–20.
Geneva Declaration Secretariat. 2008. Global Burden of Armed Violence. Geneva: Geneva Declaration Secretariat.
Ghobarah, Hazem Adam, Paul Huth, and Bruce Russett. 2003. ‘Civil Wars Kill and Maim People—Long after the Shooting Stops.’ American Political Science Review, Vol. 97, No. 2, pp. 189–202. May.
Glickman, Mark and David Van Dyk. 2007. ‘Basic Bayesian Methods.’ Methods in Molecular Biology, Vol. 404, pp. 319–38.
Guberek, Tamy, et al. 2010. To Count the Uncounted: An Estimation of Lethal Violence in Casanare. Palo Alto: The Benetech Initiative. 10 February.
Guha-Sapir, Debarati and Olivier Degomme. 2005. Darfur: Counting the Deaths— Mortality Estimates from Multiple Survey Data. Brussels: Centre for Research on the Epidemiology of Disasters. May.
Hagan, John and Alberto Palloni. 2006. ‘Death in Darfur.’ Science, Vol. 313, pp. 1578–79.
Heudtlass, Peter, Niko Speybroeck, and Debarati Guha-Sapir. 2016. ‘Excess Mortality in Refugees, Internally Displaced Persons and Resident Populations in Complex Humanitarian Emergencies (1998– 2012)—Insights from Operational Data.’ Conflict and Health, Vol. 10, No. 15.
HSRP (Human Security Report Project). 2011. Human Security Report 2009/2010: The Causes of Peace and the Shrinking Costs of War. New York: Oxford University Press.
IAEG (Inter-agency and Expert Group on Sustainable Development Goal Indicators). 2016. Report of the Inter-agency and Expert Group on Sustainable Development Goal Indicators. E/CN.3/2017/2 of 15 December.
—. 2017a. Work Plans for Tier III Indicators (as of 3 March 2017). Background document.
—. 2017b. ‘Tier Classification for Global SDG Indicators.’ 20 April.
—. 2017c. ‘Metadata for Currently Available Indicators (as of May 2017).’ IDMC (Internal Displacement Monitoring Centre). 2010. Sudan: Rising Inter-tribal Violence in the South and Renewed Clashes in Darfur Cause New Waves of Displacement. Geneva: IDMC/Norwegian Refugee Council. 28 May.
IEAG (Independent Expert Advisory Group on a Data Revolution for Sustainable Development). 2014. A World That Counts: Mobilising the Data Revolution for Sustainable Development. New York: United Nations. November.
Kleinfeld, Rachel. 2017. Reducing All Violent Deaths, Everywhere: Why the Data Must Improve. Washington, DC: Carnegie Endowment for International Peace. January.
Klingner, Jeff and Romesh Silva. 2013. ‘Combining Found Data and Surveys to Measure Mortality.’ In Taylor Seybolt, Jay Aronson, and Baruch Fischhoff, pp. 147–63.
Kruger, Jule and Kristian Lum. 2015. An Exploration of Multiple Systems Estimation for Empirical Research with Conflict-Related Deaths. Paper presented at the Visions in Methodology Conference at the University of Kentucky, 13–16 May.
Larson, Greg, Peter Biar Ajak, and Lant Pritchett. 2013. South Sudan’s Capability Trap: Building a State with Disruptive Innovation. WIDER Working Paper No. 2013/120. Helsinki: United Nations University World Institute for Development Economics Research.
Levy, Barry S. and Sidel, Victor W. 2016. Documenting the Effects of Armed Conflict on Population Health. Annual Review of Public Health, Vol. 37, pp. 205–18.
LSHTM (London School of Hygiene and Tropical Medicine). n.d. The Use of Epidemiological Tools in Conflict-affected Populations: Open-access Educational Resources for Policy-makers.
Manrique-Vallier, Daniel, Megan Price, and Anita Gohdes. 2012. ‘Multiple Systems Estimation Techniques for Estimating Casualties in Armed Conflicts.’ In Taylor Seybolt, Jay Aronson, and Baruch Fischhoff, pp. 165–82.
Obermeyer, Ziad, Christopher Murray, and Emmanuela Gakidou. 2008. ‘Fifty Years of Violent War Deaths from Vietnam to Bosnia: Analysis of Data from the World Health Survey Programme.’ BMJ, Vol. 336, No. 7659, pp. 1482–86.
OECD (Organisation for Economic Co-operation and Development). 2016. States of Fragility 2016: Understanding Violence. Paris: OECD. —. n.d. ‘Glossary of Statistical Terms.’
Pavesi, Irene. 2017. Tracking Conflict-related Deaths: A Preliminary Overview of Monitoring Systems. Briefing Paper. Geneva: Small Arms Survey. March.
Price, Megan, Anita Gohdes, and Patrick Ball. 2016. ‘Technical Memo for Amnesty International Report on Deaths in Detention.’ Washington, DC: Human Rights Data Analysis Group. 18 August.
Pritchett, Lant and Frauke de Weijer. 2010. Fragile States: Stuck in a Capability Trap? World Development Report 2011. Background paper. 5 November.
Science. 2010. ‘How Many Have Died Due to Congo’s Fighting? Scientists Battle over How to Estimate War-related Deaths.’ 21 January.
SCPR (Syrian Center for Policy Research). 2016. Confronting Fragmentation! Impact of Syrian Crisis Report. February.
Seybolt, Taylor, Jay Aronson, and Baruch Fischhoff, eds. 2013. Counting Civilian Casualties: An Introduction to Recording and Estimating Nonmilitary Deaths in Conflict. Oxford: Oxford University Press.
Silva, Romesh and Patrick Ball. 2008. ‘The Demography of Conflict-related Mortality in Timor-Leste (1974–1999): Reflections on Empirical Quantitative Measurement of Civilian Killings, Disappearances, and Famine-related Deaths.’ In Jana Asher, David Banks, and Fritz Scheuren, eds. Statistical Methods for Human Rights. New York: Springer, pp. 117–39.
Small Arms Survey. 2017. ‘A Plan of Action for Capturing the Burden of Conflict-related Deaths.’ Geneva: Small Arms Survey.
Spagat, Michael and Stijn van Weezel. 2017. ‘Half a Million Excess Deaths in the Iraq War: Terms and Conditions May Apply.’ 10 March.
Sphere Project. 2011. Humanitarian Charter and Minimum Standards in Humanitarian Response. 3rd edn. Northampton, UK: Belmont Press.
Strachan, Anna Louise, and Huma Haider. 2015. Gender and Conflict: Topic Guide. Birmingham: University of Birmingham.
Taylor, Adam. 2016. ‘The Syrian War’s Death Toll Is Absolutely Staggering. But No One Can Agree on the Number.’ Washington Post. 15 March.
UNDESA (United Nations Department of Economic and Social Affairs). 2011. United Nations Expert Group Meeting on Mortality Crises: Conflicts, Violence, Famine, Natural Disasters and the Growing Burden of Non-communicable Diseases. 14–15 November. ESA/P/WP.221. New York: UN.
UNGA (United Nations General Assembly). 2015. Resolution 70/1. Transforming Our World: The 2030 Agenda for Sustainable Development. Adopted 25 September. A/RES/70/1 of 21 October 2015.
UNHCR (United Nations High Commissioner for Refugees). 2016. Global Trends: Forced Displacement in 2015. Geneva: UNHCR. 20 June. —. 2017. Global Trends: Forced Displacement in 2016. Geneva: UNHCR. 19 June.
UNSC (United Nations Security Council). 2017. Concept Note for the Open Debate of the Security Council to be Held on 10 January 2017 on the Subject ‘Conflict Prevention and Sustaining Peace’. S/2017/6 of 5 January.
UNSG (United Nations Secretary-General). 2017. ‘Remarks to the Security Council Open Debate on “Maintenance of International Peace and Security: Conflict Prevention and Sustaining Peace”.’ 10 January.
Uppsala University. 2017. ‘New Decrease in Number of Conflict Fatalities.’ Press release. 10 May.
USDOS (United States Department of State). 2004. ‘Documenting Atrocities in Darfur.’ USDOS publication 11182. Washington, DC: USDOS Bureau of Public Affairs. September.
USGAO (United States Government Accountability Office). 2006. Darfur Crisis: Death Estimates Demonstrate Severity of Crisis, but Their Accuracy and Credibility Could be Enhanced. Report to Congressional Requesters 07-24. November.
WGMEE (Working Group for Mortality Estimation in Emergencies). 2007. ‘Wanted: Studies on Mortality Estimation Methods for Humanitarian Emergencies, Suggestions for Future Research.’ Emerging Themes in Epidemiology, Vol. 4, No. 9.
WHO (World Health Organization). 2004. Retrospective Mortality Survey among the Internally Displaced Population, Greater Darfur, Sudan, August 2004. Geneva: WHO. September.
WHS (World Humanitarian Summit). 2016. Commitments to Action. Istanbul, 23–24 May.
Widmer, Mireille. 2017a. Darfur Case Study. Unpublished background paper. Geneva: Small Arms Survey. 23 January.
—. 2017b. Indirect Conflict Deaths. Unpublished background paper. Geneva: Small Arms Survey. 1 February.
— and Irene Pavesi. 2016. Monitoring Trends in Violent Deaths. Research Note No. 59. Geneva: Small Arms Survey. September.
Wise, Paul. 2017. ‘The Epidemiologic Challenge to the Conduct of Just War: Confronting Indirect Civilian Casualties of War.’ Daedalus, Vol. 146, No. 1, pp. 139–54.
World Bank. 2017. Forcibly Displaced: Toward a Development Approach Supporting Refugees, the Internally Displaced, and Their Hosts. Washington, DC: World Bank.
About the Authors
Erik Alda is a faculty fellow in the Department of Justice, Law and Criminology at American University in Washington, DC. He holds a PhD in criminology and public policy from the same university.
Claire McEvoy is a series editor with the Small Arms Survey. Since 2001, she has worked as a research manager, researcher, and programme evaluator in fragile states in Africa, with a focus on conflict analysis, violence, protection, and gender.
Thumbnail external pageimage courtesy of Alexandr Trubetskoy/Flickr. (CC BY 2.0)
For more information on issues and events that shape our world, please visit the CSS Blog Network or browse our Digital Library.